[This article is given one + within its filename because of its carefully balanced discussion with input from experts of a legitimate concern by those jabbed which is not being accessibly reported elsewhere. –FNC]
Concerns of Lipid Nanoparticle Carrying mRNA Vaccine into the Brain: What to Make of It?
Detailing the arguments for and against this concern with input from experts.
![]()
4 days ago·[circa March 20, 2021] 12 min read
Weare all-in into vaccinating as many people as possible against Covid-19, with mRNA vaccines at the forefront. So, we might as well go all-in into understanding the little intricacies of how mRNA vaccine encapsulated by lipid nanoparticles (LNPs) might interact with delicate cell types — such as neurons in the brain — that a few experts have raised.
Before going further, the conclusion herein is that the actual risk of SARS-CoV-2 infection or Covid-19 largely outweighs the hypothetical risks of the LNP-encapsulated mRNA vaccine. But there are still a few concerns left unanswered, which deserve more transparency.
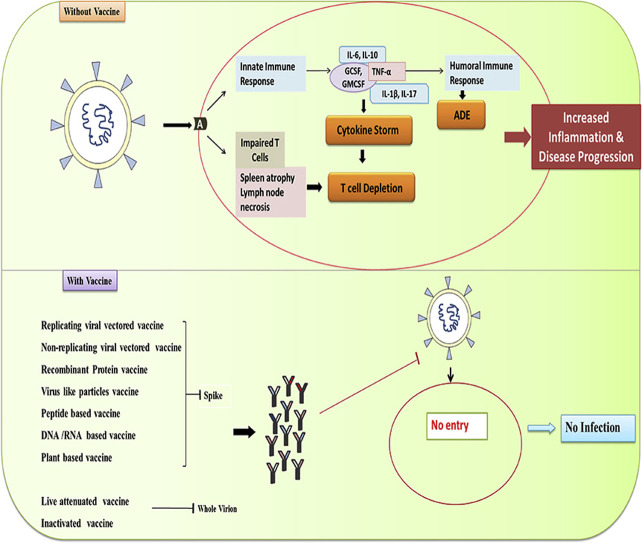
Current vaccines rely on spike protein
The
All-Vaccines-Image is from the reference just below (A 2021 Feb 5 Update re in-pipeline
COVID-19 vaccines).
Nearly all the vaccine candidates for Covid-19 — such as the
· mRNA,
· DNA,
· viral vector,
· recombinant protein,
· viral-like particles, and
· peptide-based vaccines
— rely on the SARS-CoV-2 spike protein to induce immunity.
· The Pfizer-BioNTech and Moderna mRNA vaccines consist of an mRNA genetic material encased within LNPs that can fuse with muscle and immune cells upon injection. The released mRNA then instructs the cells to make spike proteins, which are expressed on the cell surface to trigger various aspects of the immune system.
· The AstraZeneca-Oxford and Johnson & Johnson adenoviral vector vaccines use a harmless modified adenovirus to deliver DNA into the cell to make SARS-CoV-2 spike proteins to induce immunity.
· The Novavax peptide-based or protein subunit vaccine uses purified spike proteins of SARS-CoV-2 to induce immunity.
· The Sinovac and Sinopharm inactivated vaccines use dead SARS-CoV-2 virions with the spike proteins intact to induce immunity.
While these vaccines all rely on the SARS-CoV-2 spike proteins to train the immune system in one way or another, only the mRNA vaccines use the innovative LNP technology to deliver the mRNA into cells.
For simplicity, the spike protein mentioned from hereon [from here on in this article] belongs to SARS-CoV-2, the coronavirus that causes Covid-19.
Lipid nanoparticles (LNPs) hypothetical risks
The mRNA vaccine is injected intramuscularly through the arm. This method is preferred because large muscle cells have high vascularity, so the injected biomaterial can easily reach the systemic bloodstream and lymphatic system.
LNPs fuse with and enter mammalian cells easily. As mentioned, the Pfizer-BioNTech and Moderna mRNA vaccines use LNPs to encapsulate the mRNA genetic material for more efficient [intra] cell delivery.
Thus, the combined intramuscular injection and LNP technology would enable the mRNA vaccine to reach a broad range of cell types. The mRNA might even reach delicate cells or places that we don’t want them to, such as neurons in the brain or spinal cord.
In fact, LNPs are often used to overcome the problem of the BBB blocking medical drugs from entering the brain. Given that the BBB and blood-spinal cord barrier are lipid-soluble, the LNP-encapsulated mRNA vaccine might be able to enter the brain and spinal cord.
As a result, brain cells that [subsequently] express [show?] the spike protein might be marked as foreign by the [individual's own] immune system. For example, [your] cytotoxic T-cells, which kill virus-infected and cancerous cells, might see the spike protein-expressing brain cells as a threat [and kill them]. Unlike muscle cells and many other cell types, neurons in the brain rarely regenerate.
Jacob Wes Ulm, MD, Ph.D., a geneticist, explained this concern in detail in a letter to the British Medical Journal, as well as in a public comment to an article about mRNA vaccines on January 2021:
…it seems that they [mRNA vaccines] can enter a much broader tissue range compared to even attenuated virus vaccines…And since the mRNA vaccines would induce SARS-CoV-2 viral spike protein expression, that seems to mean that people who get the mRNA vaccines are going to have a much greater range of cells and tissues vulnerable to cytotoxic [T-cell] attack…with side effects that may not manifest for years (with cumulative damage and chronic inflammation).
“This is where the picture gets aggravatingly murky,” Dr. Ulm added, mentioning that there seems to be no comprehensive data on the cellular localization — i.e., which types of cells the biomaterial enters— of the LNPs used by Pfizer-BioNTech and Moderna.
Although there have been past studies on the cellular localization of LNPs (more on this below), different LNP formulations would enter different cell types, Dr. Ulm stated, so “we don’t know where in the body they’re going,” adding that:
The nightmare scenario would be if e.g. the mRNA vaccines’ lipid nanoparticles are, indeed, crossing the BBB and getting endocytosed into critical glial cells, like oligodendrocytes, or even worse, into neurons themselves in the brain and spinal cord, putting a bullseye on these critical cells for cytotoxic [T-cells].
In fact, one 2017 study vaccinated mice against influenza viruses with LNP-encapsulated mRNA vaccine. While the mRNA vaccine immunizes the mice, the study found traces of the mRNA in the brain at 0.4 ng/ml. However, the amount of mRNA found in the muscle injection site, proximal lymph nodes, distal lymph nodes, and spleen were much larger at 5680, 2120, 117, and 87 ng/ml, respectively.
That said, this is also consistent with what the European Medicines Agency’s (EMA) assessment report of the Moderna mRNA vaccine has reported:
Low levels of mRNA could be detected in all examined tissues except the kidney [in rats]. This included heart, lung, testis, and also brain tissues, indicating that the mRNA/LNP platform crossed the blood/brain barrier, although to very low levels (2–4% of the plasma level).
Therefore, these reports suggest that the LNPs can carry bits of the mRNA vaccine into the brain. But we still don’t know what would happen after the mRNA vaccine enters the brain (more on this below).
Notably, for the Pfizer-BioNTech mRNA vaccine, the assessment report by the U.K. government is a bit vague, stating that:
Information regarding the potential distribution of the test articles to sites other than the injection site following IM [intramuscular] administration has been provided and is under review as part of the ongoing rolling assessment.
Last month, I received an email from Goh Kiang Hua, MD, a consultant general surgeon, asking if I’ve come across any scientific data on what happens to the cell that makes and expresses the spike proteins upon receiving the mRNA vaccines.
I couldn’t find such any [any such], except for the abovementioned EMA’s report that I found posted in an mRNA discussion google group that William Steward, Ph.D., founded.
Dr. Ulm couldn’t either, publically commenting that:
I used to work in gene therapy and recall how we’d obsess on tissue tropism for our vectors before considering clinical trials, so I’m bewildered that this information seems almost absent for an almost entirely new vaccine modality…Without knowing more about the specific LNP formulations and their cellular and tissue trafficking patterns, we just can’t say much of anything with certainty.
Note that tissue tropism or trafficking patterns mean which tissue or cell types the biological material might enter, similar to cellular localization.
The surgeon then mentioned cases of immune thrombocytopenia — a life-threatening blood clot or platelet disorder — occurring shortly after mRNA vaccination. While no causative link has been confirmed, he considered that maybe the LNPs had carried the mRNA vaccine into the megakaryocytes (platelet-producing cells) in the bone marrow. The megakaryocytes then express the spike protein, only to be marked for destruction by cytotoxic T-cells. Platelets then become deficient, causing thrombocytopenia. Of course, he emphasized that these are just speculations.
This may be an ‘off-target effect’ of mRNA vaccines. For example, a literature review published in Pharmaceutics in January 2020 stated:
Cell-specific delivery of mRNA would be beneficial for the development of mRNA-based therapeutics. This can enhance the delivery of mRNA molecules to the targeted cells and hence reduce the required mRNA dose, as well as reducing potential off-target effects.
Overall, I see that many experts have raised hypothetical concerns of where and which cell types the LNPs might carry the mRNA vaccine into. Depending on where the mRNA ended up, the subsequent mRNA-induced spike protein expression might possibly trigger biological reactions we don’t want.
For more context about this issue, the British Medical Journal (BMJ) has also covered it last week, featuring Dr. Ulm’s concerns on the cellular localization of LNPs.
Screenshot of an article published in the British Medical Journal (BMJ) on 10th March 2021.
Why it might not be a problem
A few past studies have investigated the cellular localization of LNPs carrying an mRNA that encodes luciferase, a protein detectable via imaging scan. With this method, researchers can visually see where or which cell types the LNPs had carried the mRNA into. In a word, the luciferase visualization is a proxy for mRNA cellular localization.
· A 2015 study administered LNP-encapsulated mRNA into mice via various routes. The intramuscular route is one of the most effective ones, resulting in mRNA localization mostly in the liver and, to a lesser extent, the muscles, spleen, and lungs. The mRNA-induced luciferase protein expression peaked at about 5-hour and declined thereafter.
· A 2017 study injected LNP-encapsulated mRNA vaccine into mice and found that the mRNA disseminated mostly into the muscles, lymph nodes, spleen, and liver. But this study also found traces of mRNA in the heart, bone marrow, kidney, lung, stomach, rectum, intestines, testes, and brain. The mRNA-induced protein expression peaked at about 6-hour.
· A 2019 study injected LNP-encapsulated mRNA vaccine into macaque monkeys intramuscularly. The mRNA ended up entering the liver the most, followed by the spleen and muscles. The luciferase protein expression only lasted about 8 hours and then declined.
· A 2021 study administered LNP-encapsulated mRNA vaccine into mice via various routes, including intramuscularly. Scanning the mice's body revealed some degree of luciferase expression. While specific body parts were not mentioned, the brain didn’t appear to be one of the areas the mRNA entered. The mRNA-induced protein expression was highest within the first 24 hours and mostly gone by day 6.
Nevertheless, whether the LNP formulation of Pfizer-BioNTech and Moderna mRNA vaccines is the same as these studies remains unknown.
But we can see a trend in these studies — that intramuscular LNPs injection tends to deliver the mRNA into the muscles, liver, spleen, and lymph nodes. This cellular localization pattern is also consistent with the EMA’s assessment report of the Moderna mRNA vaccine, although they also found tiny mRNA traces in other cell types, such as the heart and brain.
Thus, we can be assured that the brain is most likely not the main tissue or organ that the Pfizer-BioNTech’s and Moderna’s LNPs enter.
In a detailed post in the mRNA discussion google group, Dr. Goh reasoned that the mRNA vaccine is unlikely to reach the brain from the arm injection site owing to the many obstacles along the way.
The mRNA vaccine would have to first escape from the densely packed muscle cells at the injection site into the lymphatic system and bloodstream. And living cells present throughout such route could take up the mRNA vaccine anytime. “Along the way, especially in the capillary beds of the lungs where the blood flow is slow, the LNPs face multiple hurdles as the whole route is lined by living cells,” he explained.
“If the LNPs survive the journey so far, the next stage is equally if not more treacherous.” The mRNA vaccine then has to resist tremendous force as the heart pumps blood throughout the body. “If the LNPs disintegrate from the turbulence, the mRNAs will be rapidly destroyed by ribonucleases,” he said. But, “those that remain intact will be sent to the WHOLE body.” Still, he further cautioned that “the structural integrity of these LNPs after being expelled from the [heart’s] left ventricle is doubtful.”
That said, here is where the brain or other organs might encounter the LNPs.
However, the brain is shielded by the BBB. So, even if the LNPs are about to enter the brain, the BBB cells could take up the mRNA vaccine, and the spike protein production might just be limited to the BBB.
Assuming the mRNA vaccine crossed the BBB successfully and entered the brain, we still don’t know what might happen after that.
Maybe the mRNA gets degraded once it enters the brain. Maybe the neurons will take up the mRNA and express spike protein on its surface, triggering cytotoxic T-cell attacks. But this is further assuming, Dr. Goh pointed out, that the T-cells would also cross the BBB. In fact, T-cell trafficking into the brain is highly regulated to prevent unwanted inflammation, so it’s not easy for T-cells to cross the BBB. The next question would be if such neuronal injury is severe enough to trigger diseases. Maybe the neuronal injury is just a little stressor that may not be detrimental health-wise.
Still, one could argue that immune cells in the brain, like microglia, might attack neurons that take up the mRNA vaccine. We know mRNA vaccine activates T-cells, but whether brain immune cells are also activated has not been studied.
It’s also worthy to note that mRNA doesn’t stay in the cell for long; it’s gone after being translated into proteins. Indeed, studies studying mRNA vaccine — in the bulleted points above — show that the mRNA-induced protein expression peaks within a few hours and then declined sharply, lasting only for a few days. As T-cells belong to the adaptive immune system, they take about 7–15 days to activate.
Dr. Goh further reminded us that participants in phase I clinical trial are still being followed up closely for nearly a year now. “This is probably the most closely watched vaccine roll-up ever in the history of vaccinology,” he stated. “To date, thankfully, there has been no signal of any long-term issues of concern.”
What to make of all this?
Overall, authorities and pharmaceutical companies may want to provide more transparency on the hypothetical concern of LNPs carrying the mRNA vaccine into areas we don’t want them to.
However, if such concerns are legitimate, it’s hard to imagine that health authorities and pharma have overlooked them. The more likely scenario may be that such concerns were considered but deemed of low concern for reasons discussed above.
Ultimately, human organ systems are complex. Theories or hypotheses alone do not always translate to the real biological phenomenon. We have seen far too many times that in vitro (test tube or cell culture) and in vivo (animal) study results failed to be replicated in humans. And these in vitro and in vivo studies are usually based on theories or hypotheses that scientists wanted to test out.
Lastly, we must also weigh the LNP mRNA vaccine's hypothetical risks against the coronavirus’s actual threats.
1. Not only is Covid-19 life-threatening among the vulnerable populations — such as older adults, people of color, and people with underlying medical conditions — but
2. long-Covid or post-Covid syndrome is another serious threat to the young and fit.
Steve Pascolo, Ph.D., co-founder of CureVac, is one of the earliest researchers to advocate for mRNA vaccines' potential in 2004. He also has an impressive publishing record on mRNA vaccines and was kind enough to respond to my email inquiring about this topic. Dr. Pascolo admits that some cells that take up the mRNA and express spike proteins on their surface might get destroyed by cytotoxic T-cells. But he added:
…that is what happens to a much higher grade and in all organs when we get infected by SARS-CoV-2…or vaccinated with live viral vaccines…With the mRNA vaccine (30 micrograms in the muscle) the eventual destruction of cells by CD8 [cytotoxic T-cells] would always be very minor compared to what happens in infection when the viruses infect virtually all cells in all organs and the immune system is fully activated to get rid of it…”
Thus, the mere 30 micrograms of mRNA vaccine injected intramuscularly pale in comparison to the actual virus infection in the capacity to trigger cytotoxic T-cell attacks in the brain or elsewhere. And yes, SARS-CoV-2 is capable of invading the brain and many other organs.
Indeed, experts in the mRNA discussion google group who first raised the hypothetical risks of LNP-encapsulated mRNA vaccines are still pro-vaccine, agreeing that SARS-CoV-2 or Covid-19 is the larger threat.
To conclude, this article doesn’t intend to undermine the mRNA vaccine but to better understand its subtle intricacies that might be important. Hopefully, there will be more research on this matter. If at all such concern is an issue, which is unlikely, we could still find ways to circumvent it. If not, then we can safely dismiss one worry we have. Either way, it’s worth knowing.
Thanks to the mRNA discussion google group — William Stewart, Ph.D., Goh Kiang Hua, MD., Christopher Shaw, Ph.D., and J. Wes Ulm, MD, Ph.D. — and Steve Pascolo, Ph.D., for their valuable input into this article.
For risk analyses of mRNA vs. Covid-19, you may be interested in this one:
Hypothetical Lasting Health Problems of mRNA Vaccine vs. Coronavirus
Neurobiology MSc postgrad in Malaysia | 2x published academic author | 100+ articles on coronavirus | Freelance medical writer |
2.1K
17
2.1K
17
· Science
· Health
· Life